文献速递:帕金森的疾病分享–使用功能性磁共振成像和机器学习预测帕金森病深部脑刺激的最优参数
Title
题目
Predicting optimal deep brain stimulation parameters for Parkinson’s disease using functional MRI and machine learning
使用功能性磁共振成像和机器学习预测帕金森病深部脑刺激的最优参数
01
文献速递介绍
常用于帕金森病(PD)的深部脑刺激(DBS)在优化后能产生显著的临床益处。然而,评估大量可能的刺激设置(即编程)需要多次诊所访问。这里,我们检查功能性磁共振成像(fMRI)是否可以用于预测个别患者的最优刺激设置。我们分析了作为观察性试验一部分前瞻性获得的67名PD患者使用最优和非最优刺激设置的3 T fMRI数据。临床上最优的刺激产生一个特征性的fMRI大脑反应模式,其通过优先激活运动回路来标记。然后,我们构建了一个机器学习模型,使用39名PD患者的fMRI模式预测最优与非最优设置,这些患者有a priori临床优化的DBS(88%准确率)。该模型预测在未见数据集中的最优刺激设置:a priori临床优化和未经刺激的PD患者。我们提出PD患者对DBS刺激的fMRI大脑反应可能代表临床反应的客观生物标志物。随着进一步通过额外研究的验证,这些发现可能为功能成像辅助的DBS编程打开大门。
Results
结果
Building on prior publications describing the safety and feasibility of MRI in DBS patients 7,9,14, 3 T fMRI data were prospectively acquired over the course of 203 fMRI sessions (n = 67 PD-DBSpatients, Fig. 1, Table 1). Since STN is the most common target for DBS in the management of PD, we primarily recruited STN DBS patients (n = 62). We also included patients with internal globus pallidus (GPi) DBS (n = 5), which is a second commonly used stimulation location, to assess whether different PD-DBS targets could also contribute to the ML model (Table 1). Each session was 6.5 min in duration and employed a 30 s DBS-ON/ OFF cycling paradigm repeated six times in which unilateral left DBS stimulation was delivered at patient-specific, clinically defined optimal and non-optimal contacts or voltages (Fig. 1C).As previously reported15, this was done to differentiate between the unilateral and contralateral BOLD signal changes, as well as to attempt to mimic DBS programming, which usually entails evaluating one electrode at a time. Acquired fMRI data were preprocessed using an established pipeline that performed motion and slice timing correction (Fig. 2). Blood-oxygen-level dependent (BOLD) signal was extracted from 16 motor and non-motor regions-of-interests (ROIs) determined a priori based on existing PET and SPECT literature16–19 and our experience with adverse effects (e.g., speech issues and visual disturbances) with non-optimal settings during DBS fMRI20. Given that fMRI studies have been uncommonly performed due to safety concerns, PET and SPECT have largely informed our ROIs choices. The absolute t-values (BOLD changes) were normalized by mean positive t-values in areas presumed to be involved in non-optimal stimulation. This was done to compare t-values of BOLD response DBS-ON vs. DBS-OFF of each ROI across patients and to account for adverse effects—a key consideration given that the aim of DBS programming is to maximize motor benefits while minimizing adverse effects. Normalized BOLD changes (features) from 39 a priori clinically optimized patients (n = 35 STN-DBS and n = 4 GPi-DBS) and their associated binary labeling (optimalvs. non-optimal) were used as input to train the ML model (Fig. 2, Table 1). Clinically optimal DBS settings were obtained using published algorithms4,5. Subsequently, two unseen fMRIdatasets (n = 9 for each dataset)—acquired with different active contacts or voltages—were fed into the trained ML model for validation purposes. The model’s ability to determine whether a DBS setting was optimal or non-optimal according to the cor responding fMRI pattern was assessed (Fig. 2).
在之前发表的有关MRI在DBS患者中的安全性和可行性的论文基础上,3 T fMRI数据在203个fMRI会话过程中前瞻性获得(n = 67 PD-DBS患者,图1,表1)。由于STN是管理PD中DBS最常见的目标,我们主要招募了STN DBS患者(n = 62)。我们还包括了内侧苍白球(GPi)DBS患者(n = 5),这是第二个常用的刺激位置,以评估不同的PD-DBS目标是否也能对ML模型做出贡献(表1)。每个会议持续6.5分钟,采用了30秒DBS-ON/OFF循环范式,重复六次,其中单侧左侧DBS刺激以患者特定的、临床定义的最优和非最优接触点或电压(图1C)提供。如先前报告所述15,这样做是为了区分单侧和对侧的BOLD信号变化,以及尝试模仿DBS编程,通常需要一次评估一个电极。获得的fMRI数据使用一个建立的流程进行了预处理,该流程执行了运动和切片时间校正(图2)。从基于现有PET和SPECT文献16-19以及我们对DBS fMRI非最优设置期间不良反应(例如,语言问题和视觉干扰)的经验,预先确定的16个运动和非运动区域感兴趣(ROI)中提取了血氧水平依赖(BOLD)信号。鉴于由于安全问题而不常进行fMRI研究,PET和SPECT在很大程度上决定了我们的ROI选择。绝对t值(BOLD变化)通过在假定涉及非最优刺激的区域的平均正t值标准化,这样做是为了比较每个ROI的DBS-ON与DBS-OFF的BOLD反应t值,并考虑到不良反应——鉴于DBS编程的目的是在最大限度地提高运动益处的同时最小化不良反应,这一点至关重要。从39个a priori临床优化的患者(n = 35 STN-DBS和n = 4 GPi-DBS)和他们的二元标签(最优与非最优)中获得的标准化BOLD变化(特征)被用作训练ML模型的输入(图2,表1)。使用已发布的算法4,5获得临床最优DBS设置。随后,两个未见fMRI数据集(每个数据集n = 9)——使用不同的活动接触点或电压获得——被输入到训练有素的ML模型中进行验证目的。该模型根据相应的fMRI模式确定DBS设置是最优还是非最优的能力被评估(图2)。
Methods
方法
Participants. Following institutional research ethics board approval (UniversityHealth Network, 14-8255), PD patients who had previously undergone DBS sur gery targeting STN or GPi at Toronto Western Hospital were enrolled in this study as a part of an ongoing observational clinical trial (Table 1, Supplementary Fig. S11, n = 67, Age = 62.9 ± 8, 41 males, 26 females; #NCT03153670, Responsible party:Andres M. Lozano, University Health Network, Toronto). GPi is also a commonly targeted structure in the management of PD1. Although both sites arguably provide similar motor benefits, there are differences: STN contributes to medication intakereduction whereas GPi may be better suited for PD patients with cognitiveimpairment and medication-associated dyskinesias55,56. Yet, the afferent and efferent circuitry for each target are different57. To assess whether different PD DBS targets could also contribute to the ML model, we explored the ML modeltraining accuracy with and without GPi-DBS patients (n = 4) (Supplementary Fig. S8). While we recruited all patients within these inclusion criteria, patients were invited to volunteer for the study and it is plausible that they may have displayed similar characteristics, for example in terms of personality and inclication to participate in trials.
参与者。**在机构研究伦理委员会批准后(多伦多大学健康网络,14-8255),之前接受过针对STN或GPi的DBS手术的PD患者被纳入本研究,作为一项正在进行的观察性临床试验的一部分(表1,补充图S11,n = 67,年龄 = 62.9 ± 8,41名男性,26名女性;#NCT03153670,负责人:Andres M. Lozano,多伦多大学健康网络)。GPi也是PD管理中常被目标定位的结构之一。尽管两个部位在提供类似的运动益处方面有论据支持,但存在差异:STN有助于减少药物摄入,而GPi可能更适合认知受损和药物相关性运动障碍的PD患者。然而,每个目标的传入和传出回路是不同的。为了评估不同的PD DBS目标是否也能对ML模型做出贡献,我们探索了包括和不包括GPi-DBS患者(n = 4)时的ML模型训练准确性(补充图S8)。虽然我们招募了符合这些入选标准的所有患者,患者被邀请自愿参加研究,他们可能显示出类似的特征,例如在个性和倾向于参与试验方面。
Fig
图
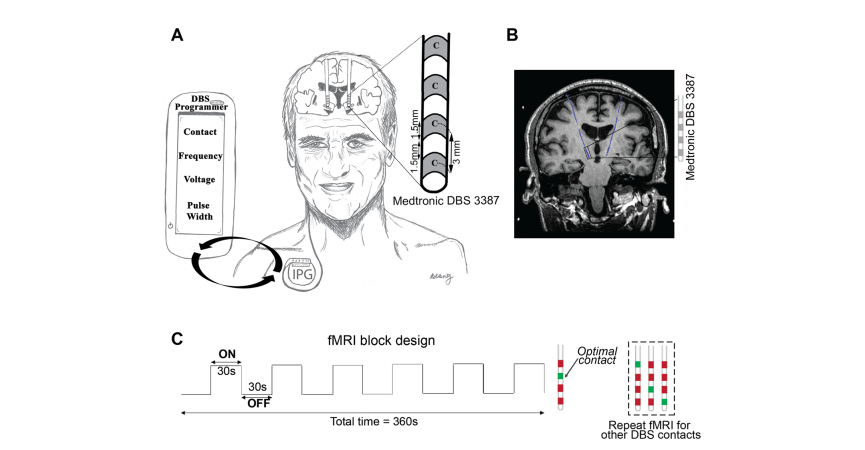
Fig. 1 Experimental design of 3 T fMRI imaging with DBS activation in PD patients. A DBS patient implanted with bilateral fully internalized and active DBS electrodes targeting the STN. The DBS lead (Medtronic 3387) has four contacts (width = 1·5 mm) spaced 1.5 mm apart. Using the handheld DBS programmer, DBS programming involves titrating the current delivered by adjusting multiple parameters (i.e., electrode contact, voltage, frequency, and pulse-width) in order to provide the best symptom relief. B Coronal T1-weighted image demonstrating a PD patient with fully internalized and active DBS electrodes (blue) implanted in the STN. C fMRI block design paradigm used during 3 T fMRI data acquisition. While the patient laid still in the scanner, unilateral (left) DBS stimulation was cycled ON and OFF every 30 s for six cycles. The DBS ON/OFF cycling was manually synchronized to fMRI
acquisition. Each fMRI sequence was acquired at either optimal (green) or non-optimal (red) contacts or voltages. In this example, the four contacts were screened with fMRI; the a priori clinically optimal contact (marked in green) and non-optimal contacts (marked in red) are shown. DBS deep brain stimulation, fMRI functional magnetic resonance imaging, PD Parkinson’s disease.
图1 PD患者进行3 T fMRI成像与DBS激活的实验设计。A DBS患者植入了双侧完全内置且活跃的DBS电极,目标是STN。DBS引导线(Medtronic 3387)有四个接触点(宽度=1·5毫米),相距1.5毫米。使用手持DBS程序器,DBS编程涉及通过调整多个参数(即,电极接触点、电压、频率和脉冲宽度)来调整所提供的电流,以提供最佳的症状缓解。B冠状T1加权图像展示了一名植入了STN中完全内置且活跃的DBS电极(蓝色)的PD患者。C在3 T fMRI数据获取期间使用的fMRI块设计范式。当患者静卧在扫描仪中时,单侧(左侧)DBS刺激每30秒循环开启和关闭六次。DBS开/关循环手动与fMRI获取同步。每个fMRI序列要么在最优(绿色)要么在非最优(红色)的接触点或电压下获取。在这个例子中,四个接触点通过fMRI筛查;事先临床上确定的最优接触点(用绿色标记)和非最优接触点(用红色标记)显示。DBS深部脑刺激,fMRI功能性磁共振成像,PD帕金森病。

Fig. 2 Summary of the methods. (Top row) After DBS surgery, PD patients undergo fMRI with fully implanted and active DBS systems. Contacts or voltages are screened and their associated fMRI patterns are fed into the machine learning model, which classifies the pattern as optimal or non-optimal. (Middle row) Pipeline for fMRI data processing. (Bottom row) Machine learning model is built with a train dataset using linear discriminant analysis and 5- fold cross validation. Then, unseen test datasets can serve as input to the model for validation. fMRI functional magnetic resonance imaging
图2 方法总结。(顶行)在进行DBS手术后,PD患者接受完全植入和活跃的DBS系统的fMRI。接触点或电压被筛查,它们关联的fMRI模式被输入到机器学习模型中,该模型将模式分类为最优或非最优。(中间行)fMRI数据处理的流程。(底行)使用线性判别分析和5折交叉验证,以训练数据集构建机器学习模型。然后,未见测试数据集可以作为输入到模型中进行验证。fMRI功能性磁共振成像。
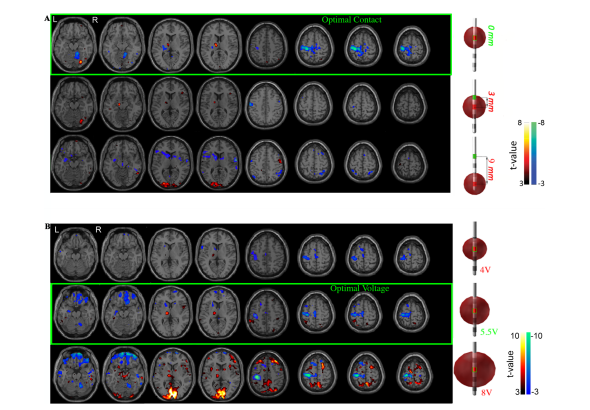
Fig. 3 Typical pattern of fMRI changes resulting from different settings. BOLD response maps associated with left DBS-STN stimulation at multiple DBS lead A Contacts and B voltages for two a priori clinically optimized PD-STN patients. The fMRI BOLD signal changes at the optimal contact (A top row) and voltage (B middle row) are shown. Brain regions with a significant increase (hot colors, positive t-values, DBS-ON > OFF) and decrease (cool colors, negative t-value, DBS-ON < OFF) (p < 0.001, cluster size = 50) in BOLD response were identified. A The optimal contact showed changes in BOLD response in the left (ipsilateral) motor cortex and thalamus, and right (contralateral) cerebellum. We considered the clinically optimal contact as the origin (i.e., 0) and the non-optimal contacts were mapped as a function of distance in mm from the optimal contact. B When using the optimal stimulation**contact, decreasing stimulation amplitude from optimal to low (subtherapeutic) voltage stimulation triggered a decrease in magnitude of the BOLD *changes but maintained the topographic pattern. High (supratherapeutic) voltages produced a relatively stronger BOLD response in the left (ipsilateral)*motor cortex and right (contralateral) cerebellum but was also accompanied by increased BOLD signal in non-motor regions such as the inferior frontal and occipital lobes. The subtherapeutic voltage was defined as 1.5 V below optimal voltage because a reduction of this magnitude yields a change in clinical status for most PD patients. The supratherapeutic voltage was defined as the voltage just below the side effects threshold (i.e., highest tolerated voltage). BOLD blood-oxygen-level-dependent, DBS deep brain stimulation, fMRI functional magnetic resonance imaging, PD Parkinson’s disease, STN subthalamic nucleus.
图3 不同设置下fMRI变化的典型模式。与左侧DBS-STN刺激相关的BOLD反应图,展示了多个DBS引导线A接触点和B电压下两名a priori临床优化的PD-STN患者。展示了在最优接触点(A顶行)和电压(B中间行)下的fMRI BOLD信号变化。识别出在BOLD反应中有显著增加(热色,正t值,DBS-ON > OFF)和减少(冷色,负t值,DBS-ON < OFF)(p < 0.001,簇大小 = 50)的脑区。A最优接触点显示在左侧(同侧)运动皮层和丘脑,以及右侧(对侧)小脑中BOLD反应的变化。我们将临床上的最优接触点视为原点(即,0),非最优接触点作为与最优接触点距离的函数映射出来。B在使用最优刺激接触点时,从最优到低(亚治疗)电压刺激的刺激幅度的减少触发了BOLD变化幅度的减小,但保持了地形图案。高(超治疗)电压在左侧(同侧)运动皮层和右侧(对侧)小脑产生了相对更强的BOLD反应,但也伴随着非运动区域如下额叶和枕叶中BOLD信号的增加。亚治疗电压定义为比最优电压低1.5 V,因为这种幅度的减少会导致大多数PD患者的临床状态变化。超治疗电压定义为刚好低于副作用阈值的电压(即,最高可忍受电压)。
BOLD血氧水平依赖,DBS深部脑刺激,fMRI功能性磁共振成像,PD帕金森病,STN丘脑下核。
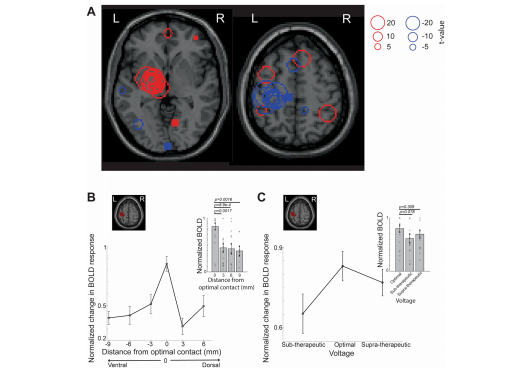
Fig. 4 Group analysis of fMRI responses to optimal DBS stimulation shows a specific response pattern. A Distribution of peak t-values overlaid on a standard Montreal Neurological Institute (MNI) brain when the clinically optimal left DBS settings are used (n = 39 total, n = 35 STN-DBS and n = 4 GPI DBS, train data). Red circles reflect increased BOLD activity (DBS ON > OFF) whereas blue circles indicate decreased BOLD activity (DBS ON < OFF). Left thalamic regions showed high overlap of peak activation t-values (DBS ON > OFF) across subjects and left motor regions showed peak deactivation t**values (DBS ON < OFF) across subjects. B The optimal contact was considered the origin (i.e., 0) and the non-optimal contacts were labeled with distances relative to the optimal contact. When the optimal contact was the most dorsal or ventral, the maximum distance to the furthest contact was 9 mm. Changes in BOLD signal in the ipsilateral primary motor cortex in response to stimulation at the optimal and non-optimal contacts on STN-DBS leads are shown. Absolute values of t-values at the left primary motor cortex ROI (shaded red) were normalized by t-values in the visual and operculum ROIs (y**axis). Mean normalized BOLD activity in the left primary motor cortex at the optimal contact was significantly different from the non-optimal contacts 3–9 mm away from optimal location (inset, n = 20 (optimal), n = 22 (3 mm), n = 13 (6 mm), n = 8 (9 mm), train data contact with at least one non-optimal contact, Table 1, two-sided Wilcoxon rank sum test). C Effects of varying voltage delivered at the optimal contact on BOLD signals are shown. Absolute values of t-values at the left primary motor cortex ROI (shaded red) were normalized by t-values in the contralateral motor cortex ROIs (y-axis). The mean normalized BOLD activity (t-values) in the left primary motor cortex (y-axis) were maximal at the left optimal contact, but not significantly different from non-optimal voltages BOLD activity (n = 19 optimal voltage, n = 15 supra-therapeutic, and n = 16 sub-therapeutic voltage settings, train data voltage (Table 1), two-sided Wilcoxon’s rank sum test). Error bars indicate SEM. Source data are provided as a Source Data file. BOLD blood-oxygen-level dependent, DBS deep brain stimulation, fMRI functional magnetic resonance imaging, ROI regions-of-interest, STN subthalamic nucleus.
图4 对最优DBS刺激的fMRI反应的群体分析显示了特定的反应模式。A在临床上最优的左侧DBS设置(总共n = 39,n = 35 STN-DBS和n = 4 GPI DBS,训练数据)使用时,峰值t值分布在标准蒙特利尔神经学研究所(MNI)大脑上的叠加。红色圆圈反映了增加的BOLD活动(DBS ON > OFF),而蓝色圆圈表示减少的BOLD活动(DBS ON < OFF)。左侧丘脑区域显示出跨受试者的峰值激活t值(DBS ON > OFF)的高重叠,左侧运动区域显示出跨受试者的峰值去激活t值(DBS ON < OFF)。B最优接触点被视为原点(即,0),非最优接触点用与最优接触点的相对距离标记。当最优接触点是最背侧或腹侧时,到最远接触点的最大距离为9毫米。显示了在STN-DBS引导线上的最优和非最优接触点处的刺激对同侧初级运动皮层BOLD信号的变化。左侧初级运动皮层ROI(红色阴影)的t值绝对值通过视觉和骨盖ROI的t值(y轴)标准化。左侧初级运动皮层在最优接触点的平均标准化BOLD活动与非最优接触点相距最优位置3-9毫米处显著不同(插图,n = 20(最优),n = 22(3毫米),n = 13(6毫米),n = 8(9毫米),训练数据接触点至少有一个非最优接触点,表1,双侧Wilcoxon秩和检验)。C显示了在最优接触点处提供的不同电压对BOLD信号的影响。左侧初级运动皮层ROI(红色阴影)的t值绝对值通过对侧运动皮层ROI的t值(y轴)标准化。左侧初级运动皮层(y轴)的平均标准化BOLD活动(t值)在左侧最优接触点处达到最大,但与非最优电压BOLD活动没有显著不同(n = 19最优电压,n = 15超治疗,n = 16亚治疗电压设置,训练数据电压(表1),双侧Wilcoxon的秩和检验)。误差棒表示SEM。源数据以源数据文件形式提供。BOLD血氧水平依赖,DBS深部脑刺激,fMRI功能性磁共振成像,ROI感兴趣区域,STN丘脑下核。
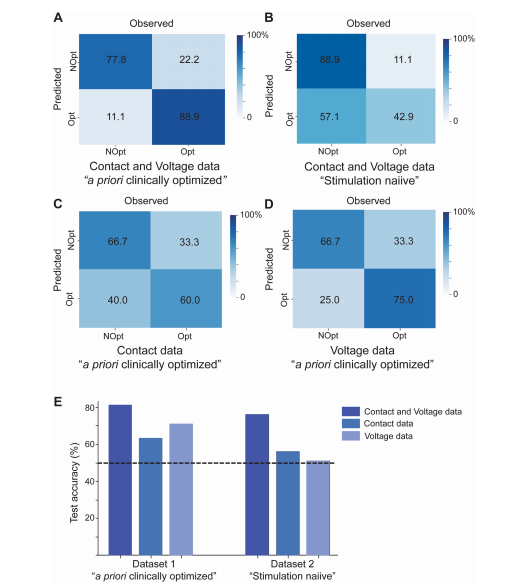
Fig. 5 fMRI responses predict optimal DBS parameters. Confusion matrices depicting the performance of classifiers trained to identify optimal DBS settings using features from A contact and voltage cohorts, C contact cohort alone, and D voltage cohort alone in an independent test set (n = 9 a priori clinically optimized patients). B Confusion matrix depicting the performance of the classifier trained to identify optimal DBS settings using features from contact and voltage cohorts in an independent test set (n = 9 stimulation naïve patients). E Summary of performance (overall accuracy) for classifiers in A–D. Bars from dataset 1 depict classifier test accuracy on n = 9 a priori clinically optimized patients. Bars from dataset 2 depict classifier test accuracy on
n = 9 stimulation naïve patients. Dashed line indicates chance at 50% accuracy. Source data are provided as a Source Data file. DBS deep brain stimulation, fMRI functional magnetic resonance imaging, NOpt non-optimal, Opt optimal.
图5 fMRI反应预测最优DBS参数。混淆矩阵展示了训练用于识别使用接触点和电压群体特征的最优DBS设置的分类器的性能,A接触点和电压群体,C仅接触点群体,和D仅电压群体在一个独立测试集中(n = 9 a priori临床优化的患者)。B混淆矩阵展示了训练用于使用接触点和电压群体特征识别最优DBS设置的分类器在一个独立测试集(n = 9未经刺激的患者)中的性能。E为A–D中的分类器性能(总体准确率)的总结。数据集1的柱状图展示了n = 9 a priori临床优化患者上的分类器测试准确率。数据集2的柱状图展示了n = 9未经刺激的患者上的分类器测试准确率。虚线表示机会水平在50%准确率。源数据以源数据文件形式提供。DBS深部脑刺激,fMRI功能性磁共振成像,NOpt非最优,Opt最优。
Table
表
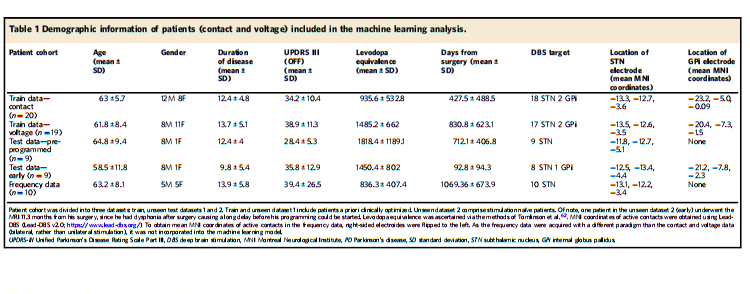
Table 1 Demographic information of patients (contact and voltage) included in the machine learning analysis
oqph-1709543559868)]
表1 包括在机器学习分析中的患者(接触点和电压)的人口统计信息